Nasal Strips: A Complete Clinical Guide (2026)
An ENT-authored, sleep-medicine-reviewed guide to how nasal strips work, who they help, who they do not, and how to use them correctly. Evidence-based and practical.


Nasal strips are one of the most commonly purchased over-the-counter devices for snoring, nasal congestion, and sleep-related breathing difficulty. They are inexpensive, widely available, and require no prescription. Despite their popularity, there is substantial confusion among patients about who they help, who they do not, and how to use them correctly.
This guide is intended as a clinical reference for adults considering nasal strips for the first time, or for those who have tried them and are unsure whether the device is the right tool for their symptoms. It covers how the strip works, the patient profiles in which it tends to be effective, the conditions for which it is not appropriate, the published evidence for and against its use, and the practical steps required to apply it correctly. Where the evidence is mixed or limited, that is stated plainly. Where the marketing tends to overpromise, the gap between claim and evidence is noted.
Key takeaways
- A nasal strip is a flexible adhesive device that exerts outward tension across the bridge of the nose, widening the narrowest segment of the upper airway, known as the nasal valve.
- The mechanical effect on nasal airflow is well established. The clinical effect on snoring is real but modest, and the device does not treat obstructive sleep apnoea.
- Strips are most useful in patients whose nasal obstruction or mild snoring originates at the nasal valve. They are not appropriate as a primary treatment for moderate to severe snoring, suspected sleep apnoea, or significant deviated septum.
- Incorrect placement is the most common reason that strips fail to work in patients who would otherwise benefit.
- Side effects are generally limited to mild, reversible skin irritation. There is no evidence that regular use causes long-term harm.
- Persistent or disruptive symptoms despite a properly conducted trial warrant clinical evaluation by an ENT or sleep physician.
What nasal strips are
A nasal strip, known clinically as an external nasal dilator, is a small flexible adhesive device worn across the bridge of the nose. It consists of one or two springy plastic bands sandwiched between adhesive fabric or polymer layers. When applied to the skin, the plastic attempts to return to its original curved shape, exerting outward tension on the soft tissue of the outer nostril walls. This widens the entrance to the nasal airway by a small but measurable amount.
External nasal dilators were introduced commercially in the mid-1990s, initially for use during athletic activity. The product category has since expanded to include indications for snoring relief, nasal congestion, and use as an adjunct to therapy for sleep-disordered breathing. Several brands are available in the Indian market, with retail prices typically ranging from ₹150 to ₹600 for a pack of 10 to 30 strips.
The continued availability of nasal strips over nearly three decades reflects the fact that, in appropriately selected patients, the device produces a measurable physiological effect. Whether that effect translates into a meaningful clinical outcome depends on the underlying cause of the patient's symptoms, which is the focus of the rest of this guide.
How nasal strips work: the nasal valve
Understanding whether a nasal strip is likely to help requires familiarity with one specific anatomical region: the nasal valve.
The nasal valve is the narrowest segment of the entire upper airway. It is located approximately one centimetre inside the nostril, at the junction between the upper lateral cartilage and the nasal septum. At this point, the cross-section of the airway resembles a thin slit. Despite occupying only a small portion of the nasal cavity by length, the nasal valve is responsible for more than half of the total resistance to airflow through the nose [1].
During inspiration, particularly forceful inspiration during sleep or exercise, the soft tissue of the outer nostril wall is drawn slightly inward by the negative pressure of inhaled air, further narrowing the valve. In some patients, this dynamic narrowing approaches partial collapse during effort, a phenomenon referred to as dynamic nasal valve collapse.
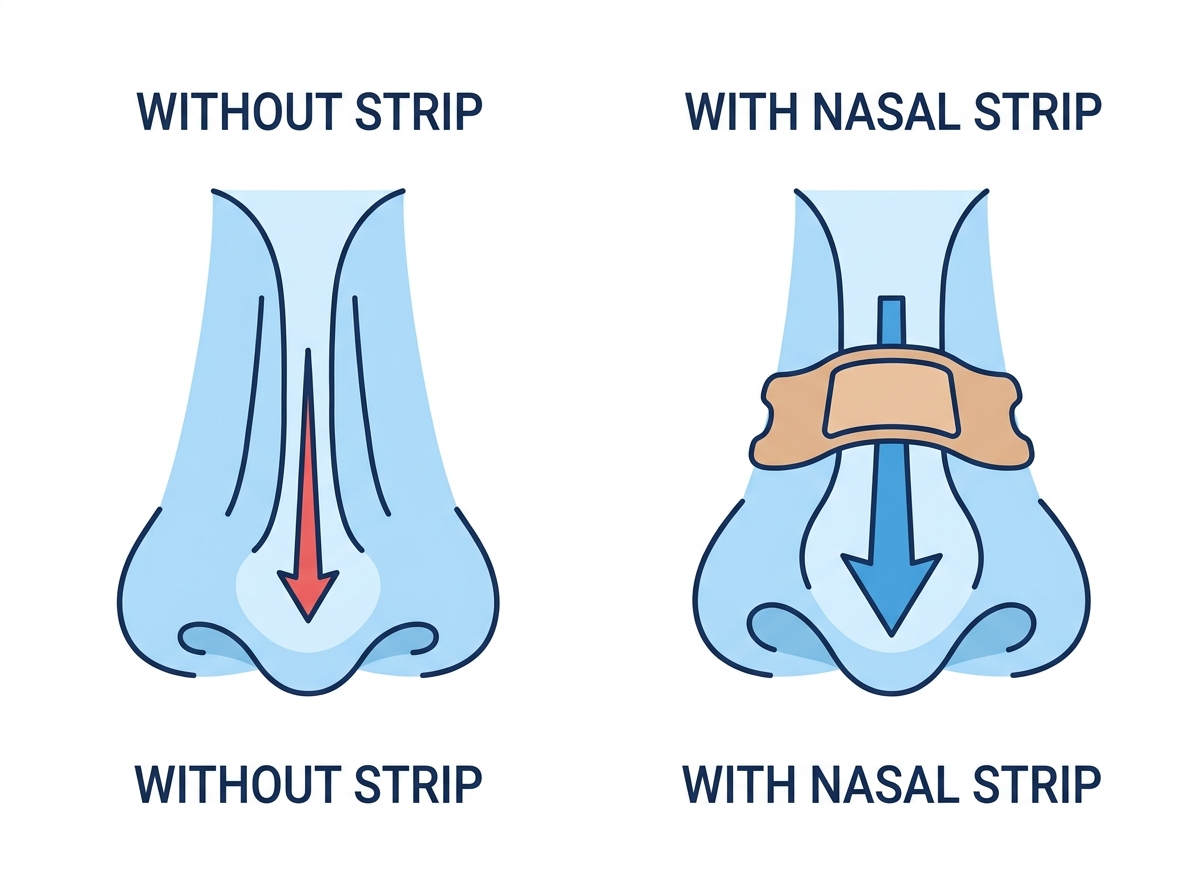
A nasal strip applies counter-tension to this region from the outside. The springy plastic band, anchored to the skin by the adhesive, exerts a gentle outward pull on the lateral nasal walls, widening the valve. Studies using acoustic rhinometry and rhinomanometry have confirmed that nasal strips increase the minimum cross-sectional area of the nasal valve and reduce nasal airway resistance in most subjects [2].
A simple bedside test, known as the Cottle manoeuvre, can identify patients likely to benefit. The patient gently pulls the cheek laterally near the side of the nose during inspiration. If breathing feels noticeably easier with this manoeuvre, the nasal valve is contributing to the obstruction, and a trial of a nasal strip is reasonable. If the manoeuvre produces no perceived improvement, the obstruction is likely further inside the nose or in the pharynx, and a strip is unlikely to help.
Who benefits from nasal strips
Nasal strips are most effective in the following clinical scenarios.
Mild primary snoring associated with nasal obstruction
In patients who snore primarily because of partial obstruction at the level of the nasal valve, widening the valve can reduce snoring intensity. Partners typically describe the snoring as softer or less continuous rather than absent. Reductions are most consistent in patients whose snoring is mild, whose snoring is not loud enough to be heard outside the bedroom, and who do not have features of obstructive sleep apnoea.
Nasal congestion from allergic rhinitis or environmental irritants
A substantial proportion of patients presenting with nasal symptoms in Indian urban centres have some degree of allergic or non-allergic rhinitis, particularly during the post-monsoon and winter months when dust mite exposure and particulate pollution peak. In these patients, the nasal mucosa is swollen, the functional cross-section of the nasal valve is reduced, and a strip can provide modest symptomatic relief at night.
A nasal strip does not treat the underlying rhinitis. It does not reduce mucosal inflammation, address allergen exposure, or substitute for medical therapy. Its role in this scenario is adjunctive, alongside measures such as dust mite control, evening saline nasal irrigation, and, where indicated, an intranasal corticosteroid spray. Patients with severe or year-round symptoms benefit from formal evaluation by an ENT specialist or allergist.
Athletic activity and exercise breathing
External nasal dilators were originally developed for use during sport. Some athletes report that nasal strips allow them to maintain nasal breathing at higher exercise intensities before transitioning to mouth breathing. The published evidence on whether strips measurably improve athletic performance is mixed. Most studies show no significant change in maximal oxygen uptake or time to exhaustion, although subjective improvements in perceived effort and respiratory comfort are more consistently reported [3].
Adjunctive use with mouth taping
Mouth taping at night has received increasing attention as a method of encouraging nasal breathing during sleep. Mouth taping is only viable when the nasal airway is patent enough to support adequate nocturnal ventilation. In patients with mild nasal valve narrowing, the combination of a nasal strip and mouth tape may be more comfortable than mouth tape alone, by improving nasal airflow capacity.
Adjunctive use with CPAP therapy
In selected patients receiving continuous positive airway pressure (CPAP) therapy for obstructive sleep apnoea, a nasal strip can improve mask comfort and may modestly reduce the required treatment pressure by lowering nasal resistance. This use should be discussed with the prescribing physician. In this scenario, the strip is an adjunct to CPAP, not a substitute.
Who nasal strips do not help
Nasal strips are not appropriate as a primary treatment in the following situations.
Obstructive sleep apnoea
Obstructive sleep apnoea (OSA) is characterised by repeated episodes of partial or complete upper airway collapse during sleep. The site of obstruction in OSA is typically at the level of the soft palate or the base of the tongue, distal to the nasal valve. Widening the nostrils does not maintain pharyngeal patency.
Untreated OSA is associated with a substantially increased risk of hypertension, cardiovascular events, stroke, metabolic complications, and daytime sleepiness severe enough to impair driving safety [4]. Patients in whom OSA is suspected, particularly those reporting witnessed apnoeas, loud disruptive snoring, unrefreshing sleep, or excessive daytime somnolence, require formal evaluation, typically with home or in-laboratory polysomnography [5]. A nasal strip is not a substitute for that evaluation.
Significant deviated nasal septum
A deviated septum that produces persistent unilateral nasal obstruction cannot be corrected by an external nasal strip, which acts only on the outer cartilaginous nasal walls. In patients with symptomatic septal deviation, septoplasty is the definitive treatment when conservative measures have failed.
Severe or year-round nasal congestion
Patients with severe or chronic nasal obstruction require diagnosis of the underlying cause. Conditions including chronic rhinosinusitis, nasal polyposis, turbinate hypertrophy, and structural anomalies each require specific treatment. A nasal strip offers, at best, minor symptomatic relief in these scenarios and may delay appropriate care if used as a sole intervention.
Loud or symptomatic snoring
Snoring that is loud, irregular, or accompanied by gasping, choking sounds, witnessed pauses in breathing, unrefreshing sleep, or daytime sleepiness should be investigated as possible obstructive sleep apnoea rather than managed with over-the-counter devices.
What the research shows
The published evidence on nasal strips can be summarised in three statements.
First, the mechanical effect is well established. Multiple studies using acoustic rhinometry and rhinomanometry have shown that external nasal dilators increase the minimum cross-sectional area of the nasal valve and reduce inspiratory nasal airway resistance in most subjects [1] [2].
Second, the clinical effect on snoring is real but modest. Early trials, including the work of Ulfberg and Fenton, demonstrated bed-partner-reported reductions in snoring intensity with Breathe Right strips in patients with primary snoring [6]. More recent and larger trials, including a 2019 study in patients with chronic nasal congestion, have shown effect sizes that are smaller and sometimes not statistically significant against placebo [7]. The most consistent interpretation is that strips can reduce mild snoring in patients whose snoring originates at the nasal valve, with no expected effect in patients with snoring of pharyngeal origin or in those with obstructive sleep apnoea.
Third, nasal strips do not treat obstructive sleep apnoea. Systematic reviews and clinical practice guidelines from the American Academy of Sleep Medicine identify continuous positive airway pressure as first-line therapy for moderate to severe OSA, with oral appliances, positional therapy, and surgical options for selected patients [5]. External nasal dilators are not recommended as a therapeutic option for OSA.
The honest summary is that nasal strips do what their physical mechanism suggests they should do. Whether that mechanical effect produces a meaningful improvement in symptoms depends on whether the patient's symptom originates at the nasal valve.
Types of nasal strips
Four broad product categories are currently available.
Standard adhesive strips. The original Breathe Right design and its many equivalents. A flexible plastic spring sandwiched between adhesive fabric layers. These are the most extensively studied, the most widely available, and the most affordable per unit. For first-time users, a standard adhesive strip in the appropriate size is the recommended starting point. Brands available in the Indian market include Breathe Right, Sanfe, Voiish, ETSAP, and Cozy.
Extra-strength adhesive strips. The same basic mechanism with a stronger spring tension. Useful for patients who experienced partial relief with the standard product but require greater outward pull. Slightly more likely to leave temporary skin marks on removal.
Magnetic strips and internal nasal dilators. Alternative mechanisms targeting the same anatomical region. Magnetic strips use small magnetic discs on each nostril, joined by a band across the bridge of the nose. Internal nasal dilators are soft silicone stents inserted into the nostrils, providing structural support from within. Internal dilators are reusable, which significantly improves cost per use over time, and may be more effective in patients in whom the obstruction is on the inner sidewall rather than the outer skin.
Reusable adhesive strips. A newer category using a tackier polymer surface intended for multiple uses across several nights. The published evidence base for this category remains limited.
For a clinically reasonable trial, a standard adhesive strip in the correct size, used for seven consecutive nights, is the appropriate starting point. If results are partial, an extra-strength version or an internal dilator is a reasonable next step.
How to use a nasal strip correctly
Incorrect placement is the single most common reason that patients who could benefit from a nasal strip report that the device does not work. In clinical practice, a significant proportion of patients who report failure of nasal strips have applied them suboptimally.
Correct application involves the following steps.
- Clean the skin. Wash the bridge of the nose with plain soap and water and pat dry. Skin oils, moisturisers, sunscreens, and cosmetics significantly reduce adhesive performance. After applying any night cream, allow at least 20 minutes for absorption before applying a strip.
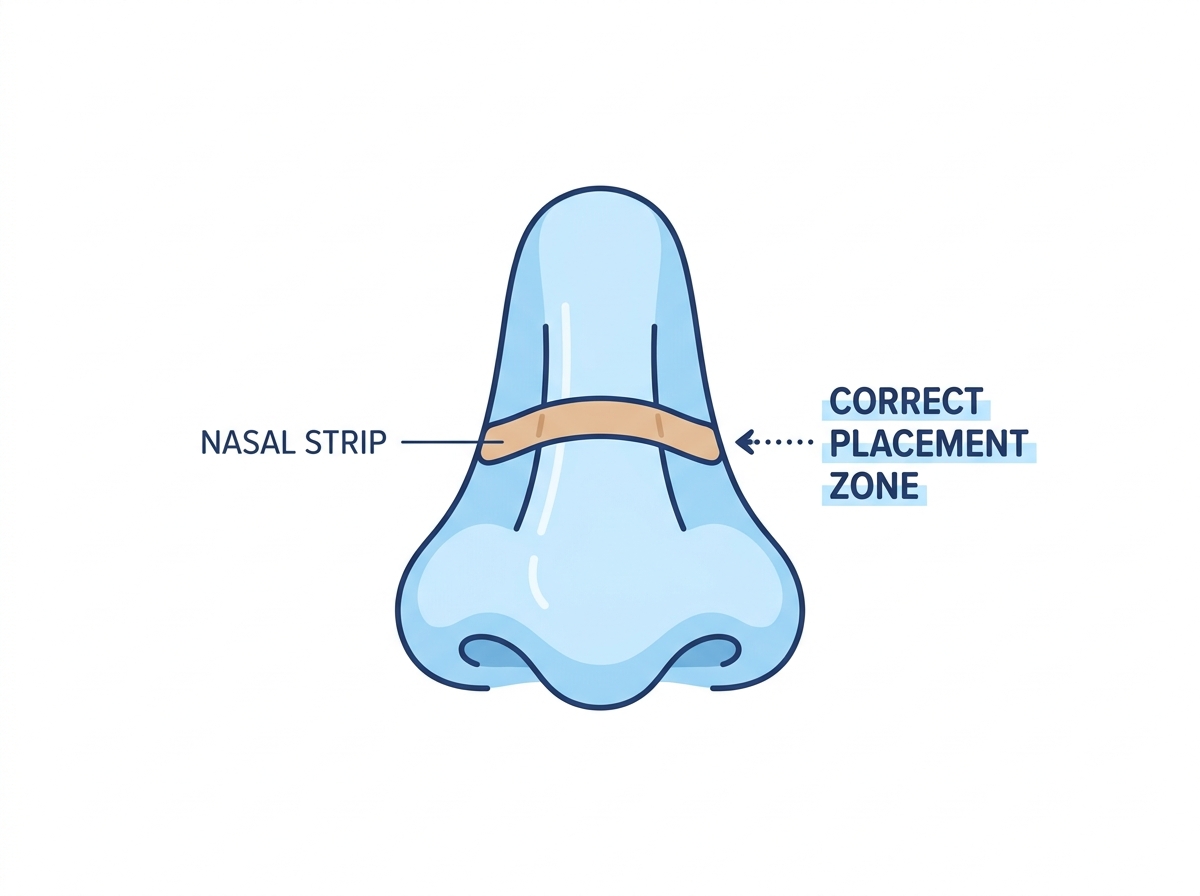
- Identify the correct position. The strip should sit on the upper portion of the nose, at the transition between the soft cartilage of the lateral nasal wall and the firmer bone of the nasal bridge. Running a finger up the side of the nose helps locate this transition. The strip belongs just below it, not at the flare of the nostril.
- Apply from the centre outwards. Place the centre of the strip first, then press down along each side. Maintain firm pressure for approximately 10 seconds to allow full adhesion.
- Confirm symmetric lift. In a mirror, both nostrils should appear slightly more open than at rest. If only one side is lifting, the strip is misaligned and should be removed and repositioned.
- Remove gently in the morning. Soften the adhesive with warm water before removal. Peel slowly in the direction of hair growth to minimise skin trauma.
A strip that detaches during sleep usually indicates either inadequate skin preparation or a prone sleeping position. Side and supine sleepers tend to retain strips more reliably than prone sleepers.
Side effects and safety
For most adults, side effects of nasal strips are minor and self-limiting. Reported adverse effects include the following.
Mild skin irritation or erythema on the bridge of the nose, usually resolving within a few hours of removal. Persistent irritation may respond to a sensitive-skin formulation or a brief break from use.
Allergic contact dermatitis to the adhesive, presenting as a well-demarcated erythematous reaction in the shape of the strip. Discontinuation and a change of brand usually resolves the issue.
Superficial skin tearing on removal, more common in elderly patients with thinner skin or in patients on topical retinoids. Wetting the strip before removal reduces this risk.
Acne exacerbation in patients with acne-prone skin, attributable to the occlusive nature of the adhesive. Varying the strip position slightly between consecutive nights and thorough morning skin cleansing usually addresses this.
Reports of more serious adverse events are rare. There is no published evidence of long-term harm from regular nightly use. The often-repeated concern that prolonged use causes "dependency" or impairs intrinsic nasal patency is not supported by clinical evidence.
When to consult a specialist
A clinical evaluation by an ENT specialist or sleep physician is recommended in the following situations.
- Witnessed apnoeas, gasping, or choking episodes during sleep
- Unrefreshing sleep or significant daytime somnolence
- Snoring that is loud, irregular, or audible outside the bedroom
- Persistent unilateral nasal obstruction
- Prior nasal trauma with subsequent change in nasal function
- No improvement after a properly conducted trial of nasal strips
- Skin reactions that persist despite a change of brand or formulation
A standard evaluation typically includes a focused clinical history, anterior rhinoscopy or nasal endoscopy, and, where obstructive sleep apnoea is suspected, formal polysomnography. The investigation does not commit the patient to surgery or to CPAP therapy. It establishes a diagnosis, which is the foundation of appropriate management.
Frequently asked questions
Are nasal strips safe to use every night?
For most adults, yes. The primary risk is mild skin irritation, which is usually reversible. There is no published evidence that nightly use of properly applied nasal strips causes lasting harm. Patients with sensitive skin should monitor for redness and consider rotating between two slightly different placement positions on alternate nights.
Will nasal strips stop snoring completely?
Generally, no. In patients with mild snoring originating at the nasal valve, strips can soften snoring intensity, and partners often report a noticeable improvement. Strips are not effective for moderate to loud snoring, for snoring of pharyngeal origin, or for snoring associated with obstructive sleep apnoea. Persistent or disruptive snoring warrants clinical evaluation rather than continued reliance on over-the-counter devices.
Can children use nasal strips?
Most commercially available strips are intended for adults. Paediatric snoring or nasal obstruction usually has identifiable causes such as adenoidal hypertrophy, allergic rhinitis, or, less commonly, structural anomalies. These require specific paediatric ENT evaluation rather than an over-the-counter device.
How long does a single strip last?
Standard adhesive strips are intended for a single overnight use. Reusable strips, depending on the manufacturer's specifications, are designed for three to seven uses before disposal. Decreased spring action, weakened adhesion, or visible deterioration of the fabric is the indication to replace the strip.
Do nasal strips help with a deviated septum?
In mild septal deviation, a strip may provide partial relief by widening the outer nostril. In moderate to severe deviation with persistent unilateral obstruction, a strip is unlikely to produce meaningful improvement, because the obstruction is internal to the cartilaginous nasal walls that the strip acts on. Septoplasty is the definitive treatment when symptoms warrant intervention.
Are magnetic nasal strips more effective than adhesive ones?
The published evidence comparing magnetic and adhesive nasal dilators is limited. For most patients, no clinically significant difference has been demonstrated. Magnetic and internal dilator formats may be preferable for patients with adhesive sensitivity, recurrent contact dermatitis, or noticeable skin marks from standard strips.
Can nasal strips be worn during the day?
Yes. There is no contraindication to daytime use. Many patients use strips during exercise or physical exertion. The mechanism of action is the same.
How much do nasal strips cost in India?
Retail prices for packs of 10 to 30 strips typically range from ₹150 to ₹600 in 2026. Indian brands are generally priced lower than imported alternatives. Bulk packs purchased online usually offer the lowest cost per strip. Cost should not be the primary basis for brand selection, as fit and adhesive tolerance vary between products.
Can nasal strips replace CPAP therapy for sleep apnoea?
No. Nasal strips do not treat obstructive sleep apnoea. In patients receiving CPAP, a strip may improve comfort by reducing nasal resistance, but it is an adjunct, not a substitute for prescribed therapy. CPAP should not be discontinued or modified without consulting the prescribing physician.
How quickly should results be apparent?
Patients who respond to nasal strips typically notice a change within the first one to three nights of correct use. A reasonable trial duration is seven consecutive nights with correctly applied strips. If no improvement is perceived after a week of correct use, a nasal strip is unlikely to be the appropriate intervention for that patient.
Are nasal strips safe during pregnancy?
Nasal congestion is common during pregnancy due to hormonal changes affecting the nasal mucosa. Nasal strips are non-pharmacological and are generally considered safe for use during pregnancy. As with any new intervention during pregnancy, brief consultation with the treating obstetrician is advisable.
Do nasal strips help with sinus headaches or sinusitis?
Nasal strips do not treat sinusitis or sinus headaches. These conditions arise from inflammation of the paranasal sinuses and require specific medical management. While a strip may incidentally improve the sensation of nasal breathing in a congested patient, it does not address the underlying sinus pathology.
Can I use a nasal strip with a cold or flu?
Short-term use during a cold can offer modest symptomatic relief from nasal congestion at night. The strip does not affect the course of the viral infection. If congestion is severe, decongestant therapy or saline irrigation are more directly effective, and should be considered first.
Bottom line
Nasal strips are a safe, inexpensive, and well-tolerated device with a clearly defined mechanism of action. Their benefit is largely confined to patients in whom partial obstruction at the nasal valve contributes to symptoms. In this group, mild snoring, nasal congestion, and exercise-related breathing difficulty may improve with use. The device is not a treatment for obstructive sleep apnoea, severe nasal obstruction, or chronic rhinitis, and should not be used as a substitute for clinical evaluation when red-flag symptoms are present.
For adults considering nasal strips for the first time, a one-week trial of a standard adhesive product in the correct size, applied correctly, is a reasonable approach. Persistent symptoms despite appropriate use should prompt formal evaluation by an ENT or sleep physician.
Medical disclaimer. The information in this article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or another qualified health provider with any questions you may have about a medical condition or treatment.