Nasal Strips for Snoring: Do They Really Work? (2026)
An ENT-authored, sleep-medicine-reviewed guide on whether nasal strips actually reduce snoring, who they help, what the evidence shows, and when to see a specialist instead.


Snoring is one of the most common reasons adults look for an over-the-counter sleep aid. Nasal strips are usually the first product they try, often after a partner has lost patience with the noise. The strips are inexpensive, easy to find, and require no prescription. The question most patients arrive with, however, is the right one to ask: do they actually work?
The honest answer is that nasal strips help some snorers, do not help others, and are sometimes used in place of evaluation that the patient actually needs. Whether they will help in a specific case depends almost entirely on where the snoring originates anatomically. This guide explains the difference between nasal-origin and pharyngeal-origin snoring, summarises the published evidence on strips for snoring, and lays out the patient profiles in which strips are most and least likely to produce results.
Key takeaways
- Nasal strips can reduce snoring in patients whose snoring originates at the nasal valve, where partial obstruction creates the airflow turbulence that produces the snoring sound.
- They are unlikely to reduce snoring that originates further back in the airway, at the soft palate or base of the tongue, which is where most loud, persistent snoring comes from.
- The published evidence shows modest, inconsistent reductions in snoring intensity with nasal strips. Some patients respond well. Others see no benefit.
- Loud, irregular snoring with daytime sleepiness, witnessed pauses in breathing, or choking sounds may indicate obstructive sleep apnoea, which strips do not treat.
- A simple one-week trial of a correctly applied standard adhesive strip is the most reasonable way to decide whether the device will help an individual patient.
Why people snore: a short anatomical primer
Snoring is the sound produced when air flowing through the upper airway during sleep causes soft tissue to vibrate. Three conditions together generate the sound: airflow under pressure, a partly narrowed airway, and soft tissue that can flutter. Remove any one of these, and the snoring stops or softens.
During sleep, the muscles that hold the upper airway open relax. The tongue falls slightly backward. The soft palate, the cheeks of the throat, and the tissues of the back of the nose can all loosen enough to vibrate when air rushes past them. The narrower the airway, the more forcefully a person has to inhale, and the louder the resulting vibration. This is why snoring is usually worse when sleeping on the back, after alcohol, or when a person is congested.
Not all snoring is the same, and not all snoring responds to the same intervention. The most important question is where in the airway the snoring originates.
The two sites where snoring originates
There are two anatomical regions responsible for the great majority of snoring.
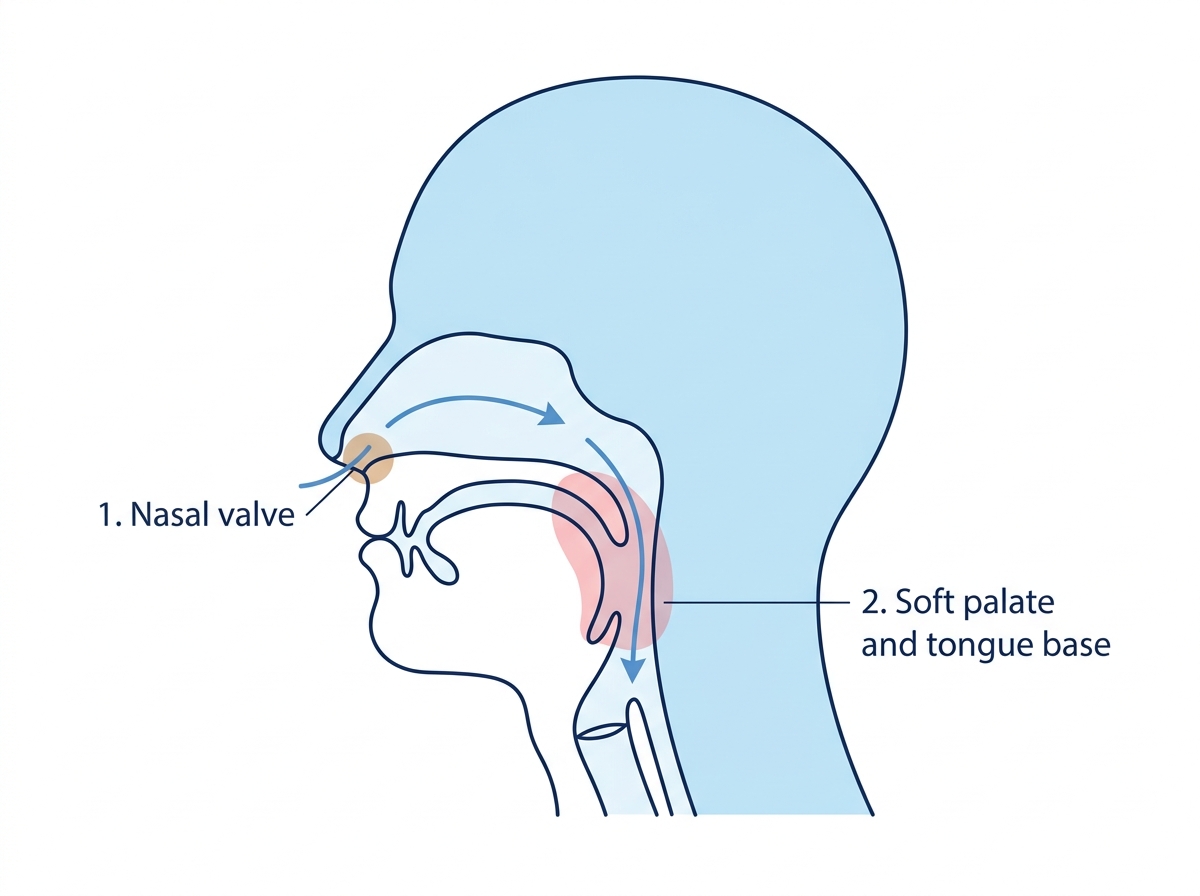
1. The nasal valve
The nasal valve is the narrowest segment of the entire airway and is located approximately one centimetre inside the nostril, where the upper lateral cartilage meets the nasal septum. Despite occupying only a small portion of the nasal cavity, it is responsible for more than half of the total resistance to airflow through the nose [1].
When the nasal valve is partly obstructed, by mucosal swelling, dynamic collapse of the outer nostril wall during inspiration, or anatomical narrowing, the patient has to inhale more forcefully to draw the same amount of air. That forceful inhalation, in turn, increases the negative pressure further down the airway and can set the soft palate and other downstream tissue vibrating.
In snoring of nasal-valve origin, fixing the bottleneck at the nasal valve reduces the negative pressure further down and, often, reduces the snore. This is the mechanism by which nasal strips help certain patients.
2. The soft palate and base of the tongue
The second site is in the pharynx, behind the mouth, where the soft palate, the uvula, the tonsillar pillars, and the back of the tongue form a flexible muscular tube. During sleep, this region tends to relax and partially collapse, and the resulting narrowing is where most loud, position-related snoring originates.
Snoring of pharyngeal origin is generally not improved by nasal interventions. Widening the nostrils does not change what is happening at the back of the throat. This region also happens to be the same site where the airway collapses fully in obstructive sleep apnoea, which is why pharyngeal snoring deserves a closer look from a clinician.
In clinical practice, the distinction between these two anatomical patterns is what determines whether a nasal strip is worth trying.
How nasal strips reduce snoring (when they work)
A nasal strip is a flexible adhesive band worn across the bridge of the nose. Its springy plastic core pulls outward on the soft tissue of the outer nostril walls, widening the nasal valve by a small but measurable amount. Studies using acoustic rhinometry and rhinomanometry have confirmed that external nasal dilators increase the minimum cross-sectional area of the nasal valve and reduce inspiratory nasal airway resistance [2].
When the obstruction contributing to snoring is at the nasal valve, this small widening can produce a meaningful clinical change. Patients describe the strip in one of two ways. Either they breathe more easily on awareness, which often translates into reduced snoring volume, or their bed partner reports that the snoring is softer or less continuous through the night.
The effect is modest. Strips do not eliminate snoring. They do not reach the throat. What they can do is reduce one specific input, the nasal contribution, which in the right patient is enough to shift the snoring from disruptive to tolerable, or, occasionally, to absent.
What the research shows
The literature on nasal strips for snoring is real but limited, and the marketing tends to overpromise relative to the evidence.
Early studies, including the work of Ulfberg and Fenton, reported bed-partner-observed reductions in snoring intensity with Breathe Right strips in patients with primary snoring [3]. A 1998 trial in primary snorers found measurable decreases in snoring duration and intensity for a majority of participants, although the magnitude of the effect varied widely between individuals.
More recent and larger studies have shown smaller effect sizes. A 2019 study examining the role of nasal dilator strips in sleep-disordered breathing concluded that strips produce variable improvements in subjective sleep and snoring outcomes, with the strongest responses in patients whose primary obstruction was clearly at the nasal valve [4]. Systematic reviews have concluded that external nasal dilators may modestly reduce snoring in selected patients but should not be considered a primary treatment.
For obstructive sleep apnoea (OSA), the evidence is consistent in the opposite direction. Strips do not treat OSA. They do not reduce the number of apnoeic events. American Academy of Sleep Medicine guidelines identify positive airway pressure as the first-line therapy for moderate to severe OSA, with oral appliances, positional therapy, and surgery for selected patients [5]. External nasal dilators are not listed as a therapeutic option for OSA in current guidelines.
The clinically honest summary is that nasal strips work when the snoring is nasal in origin and do not work when it is not.
Who is most likely to benefit
Based on the published evidence and routine clinical assessment, patients most likely to see a meaningful response to nasal strips share several features.
- Snoring is mild and primary. The snoring is audible to a bed partner but not to someone in another room, and is not associated with witnessed pauses, gasping, or daytime sleepiness.
- There is a nasal contribution. The patient reports a sense of nasal obstruction, congestion, or restricted breathing through the nose, particularly at night.
- The Cottle manoeuvre is positive. Gently pulling the cheek laterally near the side of the nose during inspiration produces a perceptible improvement in nasal breathing. This is a simple bedside test for nasal valve dysfunction.
- There are no red-flag features. No history of witnessed apnoeas, no choking arousals, no unrefreshing sleep, no excessive daytime sleepiness.
- Body mass index is in a healthy range. Obesity is an independent risk factor for both snoring and sleep apnoea, and patients with significant obesity are less likely to respond to a nasal intervention alone.
In this profile, a one-week trial of a correctly applied nasal strip is a reasonable first step. Improvement is usually noticeable within one to three nights of correct use.
Who is unlikely to benefit
Some patient profiles are unlikely to respond to a nasal strip and should be evaluated for alternative interventions.
- Loud, persistent snoring audible from another room suggests substantial pharyngeal contribution and warrants clinical evaluation, not a strip.
- Witnessed pauses in breathing, choking, or gasping during sleep are red flags for obstructive sleep apnoea. A sleep study is the appropriate next step.
- Daytime sleepiness or unrefreshing sleep, particularly with snoring, raises suspicion for OSA and should not be managed with over-the-counter devices.
- Significant deviated septum with persistent unilateral nasal obstruction is unlikely to respond meaningfully to a strip. Septoplasty is the definitive treatment if symptoms warrant it.
- Obesity and large neck circumference are associated with pharyngeal-origin snoring and a higher likelihood of OSA. Weight management and a sleep evaluation usually take precedence over over-the-counter devices.
- A negative Cottle manoeuvre suggests the obstruction is not at the nasal valve, and a strip is unlikely to help.
In all these cases, the right next step is a clinical evaluation rather than continuing to try different brands of strips.
Best types of nasal strips for snoring
Patients often ask which specific brand or type of strip is most effective for snoring. The honest clinical answer is that for most patients, the differences between major branded strips are smaller than the differences between correct and incorrect placement, or between an appropriate and an inappropriate patient profile. That said, the products available in the Indian market in 2026 fall into four broad categories.
Standard adhesive strips. The original Breathe Right design and its many equivalents. A springy plastic band sandwiched between adhesive fabric layers. These are the most extensively studied and remain the first-line product for most patients. Indian brands available include Breathe Right, Sanfe, Voiish, ETSAP, and Cozy. Choose a size that comfortably covers from one outer nostril to the other.
Extra-strength adhesive strips. The same mechanism with a stronger spring. Useful for patients who experienced partial relief with the standard product but want more outward pull. Slightly more likely to leave temporary skin marks on removal.
Magnetic nasal strips. A different mechanism using small magnetic discs on each nostril, joined by a band across the bridge. Some patients find these more comfortable, particularly those with skin sensitivity to adhesives. The published evidence comparing magnetic and adhesive strips for snoring reduction is limited.
Internal nasal dilators. A soft silicone stent inserted into each nostril, providing structural support from within. Internal dilators are reusable, which reduces the cost per use over time, and may be effective in patients in whom the obstruction is on the inner sidewall of the nostril rather than the outer skin. They take some getting used to but are well tolerated by most.
For first-time users, a standard adhesive strip in the correct size, used for seven consecutive nights, is the appropriate trial. If results are partial, an extra-strength version or an internal dilator is a reasonable second step before concluding that the device does not help.
How to use a nasal strip effectively for snoring
Strips fail more often because of incorrect application than because of an inappropriate patient. The following steps maximise the chance that the device will actually work.
- Clean and dry the skin. Wash the bridge of the nose with plain soap and water and pat dry. Skin oils, moisturisers, sunscreens, and night creams reduce adhesion significantly. If a night cream has been applied, allow at least 20 minutes for absorption before placing a strip.
- Place the strip high on the bridge, not on the flare. Run a finger up the side of the nose. There is a transition point where the soft cartilage meets the firmer nasal bone. The strip belongs just below this transition, not down at the flare of the nostril. Misplacement is the most common reason for non-response.
- Press from the centre outwards. Apply the centre of the strip first, then press down along each side. Hold firm pressure for about ten seconds.
- Check for symmetric lift. Both nostrils should appear slightly more open than before. If only one side is lifting, reposition the strip.
- Sleep on the back or side rather than the stomach. Prone sleepers tend to dislodge strips by pressing the face into the pillow. Side and supine sleepers retain strips more reliably.
- Remove gently in the morning. Soften the adhesive with warm water first, then peel slowly in the direction of hair growth to minimise skin irritation.
A one-week trial under these conditions is a fair test of whether the strip can help an individual patient. If snoring has not changed at all by the end of seven nights of correct use, the strip is unlikely to be the right tool, and other interventions should be considered.
When snoring is more than snoring: red flags for sleep apnoea
Obstructive sleep apnoea is a distinct medical condition characterised by repeated partial or complete collapse of the upper airway during sleep, with associated drops in oxygen levels and brief arousals from sleep. OSA is common, underdiagnosed in India, and associated with substantially increased risk of hypertension, cardiovascular disease, stroke, and accidents related to daytime sleepiness [6]. It also has a strong familial component and is more common with increasing age, weight, and neck circumference.
Snoring is the most common symptom of OSA, but most snorers do not have OSA, and most importantly, OSA cannot be diagnosed from snoring alone. The features that suggest a clinical evaluation is needed include:
- Loud snoring audible outside the bedroom
- Witnessed pauses in breathing during sleep, often noticed by a bed partner
- Choking or gasping arousals
- Unrefreshing sleep, irrespective of duration
- Excessive daytime sleepiness or fighting sleep during routine tasks
- Morning headaches
- Difficulty with concentration or memory
- Recently diagnosed or poorly controlled high blood pressure
If any of these are present, the appropriate next step is not another packet of nasal strips. It is a sleep evaluation, which usually starts with a clinical history, a focused examination, and often a sleep study that can be done at home in many cases.
When to see an ENT or sleep physician
Beyond the OSA red flags above, an in-person consultation is appropriate in the following situations.
- Snoring that has worsened over weeks or months, particularly if associated with weight gain
- Persistent unilateral nasal obstruction
- Nasal trauma followed by a change in nasal function or snoring pattern
- Failure of a properly conducted one-week trial of correctly applied nasal strips
- Skin reactions to multiple brands of strips
- Snoring in a child or adolescent, which has different causes and should never be self-managed with adult over-the-counter products
A standard evaluation includes a focused history, anterior rhinoscopy or nasal endoscopy, and, where indicated, polysomnography. The investigation does not commit a patient to surgery or to CPAP therapy. It establishes a working diagnosis, which is the foundation of appropriate management.
Frequently asked questions
Do nasal strips actually stop snoring?
They reduce snoring in some patients and do not in others. Patients with mild snoring of nasal origin are most likely to respond. Patients with loud, persistent snoring of pharyngeal origin, or with obstructive sleep apnoea, are unlikely to respond.
How quickly will I notice a difference?
Patients who respond usually notice a change within the first one to three nights of correct use. A reasonable trial duration is seven consecutive nights. If there is no change at all by then, the strip is unlikely to be the right intervention.
Can my partner tell if the strip is working before I can?
Often, yes. Bed-partner observations are usually more reliable than self-report for snoring, because the snorer is asleep when it happens. Asking a partner for an honest assessment over the trial week is more useful than relying on the patient's own impression.
Are nasal strips safe to use every night?
For most adults, yes. Mild skin irritation is the most common adverse effect and is usually reversible. There is no evidence that nightly use of properly applied strips causes lasting harm.
Can children use nasal strips for snoring?
No, not without paediatric evaluation. Snoring in children most often relates to adenoidal hypertrophy, tonsillar enlargement, allergic rhinitis, or, less commonly, structural causes. These require specific paediatric assessment, not over-the-counter devices.
Do nasal strips help if I snore only when I drink alcohol?
Alcohol relaxes the muscles of the upper airway and worsens pharyngeal snoring. Nasal strips do not counter this effect. The most reliable intervention for alcohol-related snoring is to avoid alcohol close to bedtime.
Will nasal strips help if I sleep on my back?
Position-related snoring is usually pharyngeal in origin and responds best to changing sleep position rather than to a nasal strip. Side sleeping reduces the gravitational collapse of pharyngeal tissue. A strip may help if there is an additional nasal component.
Are magnetic nasal strips better for snoring than adhesive ones?
The published evidence comparing magnetic and adhesive strips specifically for snoring reduction is limited. For most patients, neither has a clear advantage over the other. Magnetic and internal dilator formats are most useful for patients with adhesive sensitivity.
Can nasal strips replace CPAP therapy?
No. Nasal strips do not treat obstructive sleep apnoea. In patients on CPAP, a strip can occasionally improve mask comfort and reduce required pressure by lowering nasal resistance, but it is an adjunct only.
What if the strip falls off in the night?
Usually this indicates either inadequate skin preparation (oils, moisturisers, sweat) or a prone sleeping position. Clean the bridge of the nose thoroughly before application, allow night creams to absorb fully, and try a side or supine sleeping position. If the strip continues to detach, consider an extra-strength version or an internal dilator.
How much do anti-snoring nasal strips cost in India?
Retail prices typically range from ₹150 to ₹600 for packs of 10 to 30 strips. Indian brands are generally less expensive than imported alternatives. Cost should not be the primary basis for selection, since fit and adhesive tolerance vary between products.
What is the best long-term solution for snoring if strips do not work?
The right long-term answer depends on the underlying cause. For pharyngeal-origin snoring, positional therapy, weight management, addressing alcohol or sedative use, and treatment of any underlying OSA are the foundations. For structural nasal obstruction, septoplasty or turbinate procedures may be appropriate. The best path forward starts with a clinical evaluation rather than a search for a better over-the-counter product.
Bottom line
Nasal strips reduce snoring in patients whose snoring originates at the nasal valve. They do not reliably help when snoring originates further back in the airway, and they do not treat obstructive sleep apnoea. The published evidence supports a modest, variable effect with the strongest responses in patients selected on clinical features that suggest a nasal contribution to the snoring.
For an adult with mild snoring, no red-flag features, and a sense of nasal obstruction at night, a one-week trial of a correctly applied standard adhesive strip is a reasonable first step. If results are clear and helpful, continued use is safe. If results are partial, an extra-strength or internal dilator product is the next reasonable trial. If results are absent or if any red-flag features are present, the right next step is a clinical evaluation by an ENT or sleep physician, not another brand of strip.
Medical disclaimer. The information in this article is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the guidance of your physician or another qualified health provider with any questions you may have about a medical condition or treatment.